











The much-recommended measure of social distancing practised around the globe to stem the spread of this pandemic is almost impossible in many parts of India
When pandemics hit, they usually hit the poor the hardest, if not the first. Like the months bygone, the next couple of months are going to schlep through the looming threat of the contagion bulging into the next stage of community spread. This may precipitate the exponential disease spikes and deaths in numbers that we can very well speculate. They may be in thousands if not millions, considering the poverty and density of population. It is high time that we stand up and walk with the Government and aid its efforts to fight the pandemic by not only following its instructions on social distancing and not hoarding essential commodities but also by contributing intelligent observations and suggestions.
We have seen so far that COVID-19 can quickly overwhelm the health systems of countries, including those nations that are said to have advanced healthcare systems, like Italy and the United States (US). The ongoing rise in mortality in such developed nations portends a very dark future for poorer nations with inadequate healthcare facilities, including ours.
The first line of defence against any pandemic is surveillance: Monitoring human (and animals where relevant) populations to spot outbreaks and containing them at the earliest. In countries with overall impoverished infrastructure, isolated outbreaks are likely to go undetected longer and thus simmer and spread.
At the current stage, our public healthcare system is expected to detect where the virus is spreading and collect high-quality real-time data from various geographies and groups of people, identifying pockets of infection before they multiply into larger outbreaks.
It is for our health systems to be able to figure out which communities can expect to see a rise in Coronavirus cases and where to allocate resources in anticipation of rising hospitalisations.
Without quality data, no one can respond appropriately to this fatal threat, neither as individuals nor as a society. Nor can we learn whether countermeasures adopted so far against the pandemic are working or not. The most important component of the contagion data is information from the laboratory tests detecting active infections, past infections, immunity status of people as well as assessing herd immunity in communities. These present a real picture of the Coronavirus’ spread and status in the country.
The priorities of action plans for the road back to normalcy would be maintaining a robust and vigilant healthcare system, a firm administration with impeccable attention to detail regarding the nuances of the vulnerable groups living at the edges (migrants and daily wage labourers) and an effective targetted (sentinel) surveillance system.
If the country’s systems function to their full potential, we would be able to learn where the Coronavirus is dormant. And once we know the location and size of the problem, we can start leaving our homes gradually, return to work and attend schools and universities, bring businesses back in shape and let people congregate for movies, meetings, weddings or mass prayers.
An observation, or rather a lesson learnt from countries battling the Coronavirus in an advanced stage than ours, is that the threats posed by the virus have cast a spotlight on the shortcomings in healthcare systems across the globe. The population of billions in India may be the next battleground in the fight against the contagion if proactive measures are not undertaken at this stage.
Home to one-third of the world’s slum-dwelling population, India is largely filled with people battling poverty and poor education (including health education and general inadequate know-how about things), existing co-morbid conditions and most importantly hygiene challenges (i.e., limited access to resources such as clean water, soap, disinfectants and so on).
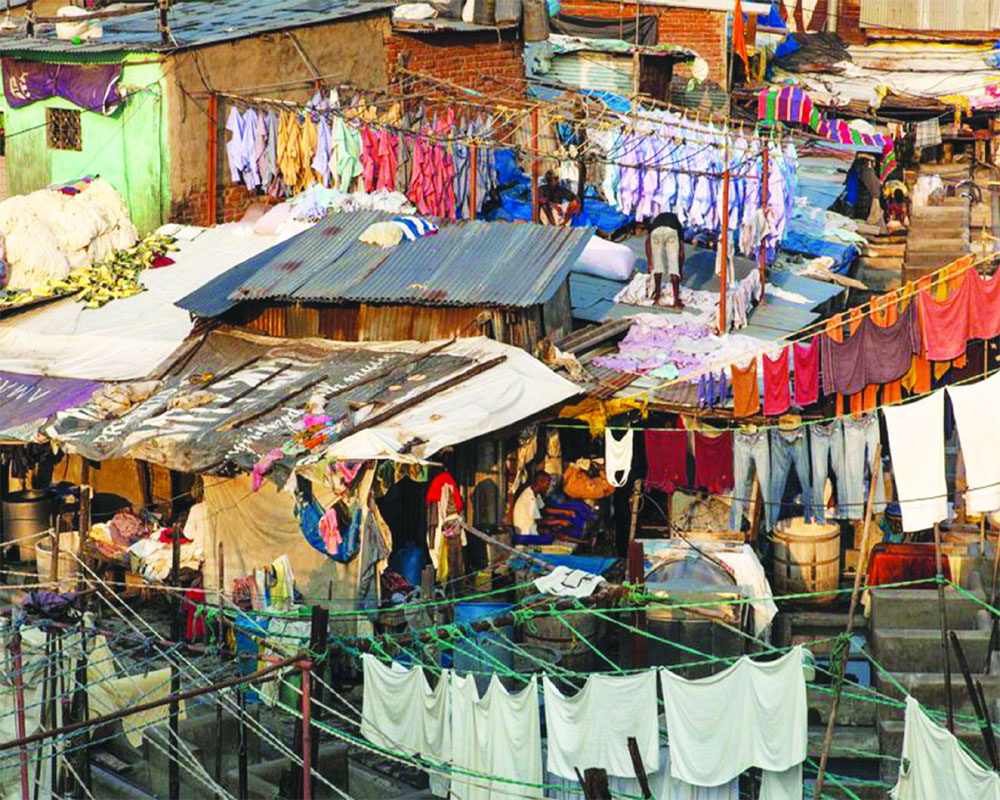
The much-recommended measure of social distancing practised around the globe to stem the spread of this pandemic is almost impossible in many parts of India. With a population density of 2,77,136 people per square kilometre (sq km) in Mumbai’s Dharavi slum to 1,25,000 people per sq km at the Rasoolpura slum in Hyderabad, the difficulty in observing social distancing is self-explanatory. Slums are an integral part of a city’s economy as those are where a majority of the labour force and domestic help stays, all around the country. Now, with three cases of Coronavirus cases appearing in the Dharavi slum, these places are also a ticking time bomb where the contagion is concerned.
The biggest challenge regarding hygiene is overcrowding around common toilets — Dharavi slum has one toilet per 1,440 residents. The Covid-19 virus is known to survive longer than three days in faecal matter, which makes crowding around toilets and living amid bad drainage a major threat.
The focus must now shift to proactive testing for asymptomatic and symptomatic Covid-19 bearers, within the most vulnerable, high population density pockets of India.
There are genuine capacity issues but we need mandatory Covid-19 testing of all slum inhabitants across the country. Quarantine is a must for the asymptomatic and symptomatic bearers of the Coronavirus in slum zones in different pre-identified, isolated locations.
This test data is vital in enabling the right strategy to manage the next steps of Coronavirus containment and eradication. The health system hence should encourage doctors to test liberally (without any out-of-pocket payment from the people given their economic status).
About laboratory test data, we see that unlike in developed nations, the data is either incomplete or completely unavailable in developing nations like ours due to poor infrastructure and coordination issues. This makes it impossible for administrators, scientists, healthcare professionals, researchers and the general citizen to assess the extent and significance of the testing efforts.
The other component of an effective healthcare system of a low-income country is to focus on serology tests. RT-PCR is the confirmatory test for COVID-19 which is currently priced at Rs 4,500 per test and takes more than a day for the result to be available. The serology tests on the other hand are much cheaper and can be used extensively for screening. These are not confirmatory tests and hence not used in clinical practice but these tests have value in epidemiology studies and herd immunity assessment.
These tests screen blood for the antibodies that confer immunity after exposure to a pathogen. In public health management, this is essential for tailoring interventions and stopping local spread of a disease, especially a contagious one. Serology is uniquely useful for defining specific anti-viral immunity. If you know that a large percentage of people have been exposed and developed some immunity, it may allow for less-restrictive measures. These tests can be added to routine blood draws with no additional hassle for the patient.
For instance, in the US, ever since the Coronavirus outbreak began, many different groups have ramped up their efforts to develop a serological test. Should a test like this ever become available to the public, it could radically shape how healthcare professionals decide who gets to leave home and return to some semblance of a normal life.
Considering the current status of the Coronavirus contagion, with the uncovering of 10 hotspots of the viral infection within the country, a sentinel surveillance system must now exist in full force and to the highest accuracy.
The Government needs to build it with dedicated funding, perhaps as part of the next stimulus package. This will require an efficient data-collection system that allows cases/suspected hotspots of the disease to be identified and tracked in real time (without overburdening providers with data entry and case reports).
Many of our citizens have already called for the need for special financing arrangements to support surveillance and preparedness for the worst-case scenario of a fierce outbreak. They have also underscored the importance of incentivising the right type of capacity-building, including the right research and evidence-generation capability, to enable effective containment of infection and other mitigation strategies. With funds coming in from various sources and from the taxpayers’ money that is directed towards the COVID-19 response, India, even with a weak healthcare system should concentrate on this and use all available resources wisely until we come out of the pandemic, bruised but not totally defeated.
(The writer is an author and a doctor by profession)












